
What The Pitt Gets Right About the U.S. Health Care System
LDI Fellows Weigh in on the HBO Max Show, Describing Real Challenges From High Patient Bills to Assaults on Nurses in the ER
Health Equity | Population Health
News
Incarceration is a large-scale social determinant of health, with broad and enduring dynamics that produce long-term health damage far beyond prison walls, argued LDI Senior Fellow Jason Schnittker, PhD, at an April 7 University of Pennsylvania seminar titled “Behind Bars, Beyond Health: Equity and Incarceration in America.” The event was part of Penn Medicine’s 11th Annual Health Equity Week, organized by the Center for Health Equity Advancement.
Schnittker, a Professor of Sociology at Penn’s School of Arts and Sciences, is also co-author of the 2022 Oxford University Press book, “Prisons and Health in the Age of Mass Incarceration.”
Presenting in the auditorium of Penn’s Leonard Davis Institute of Health Economics (LDI), Schnittker emphasized that it is not well appreciated that incarceration is not just a criminal justice issue, but also a major population health issue that undermines the health of people currently and formerly in prison as well as their families, communities, and larger health care systems.
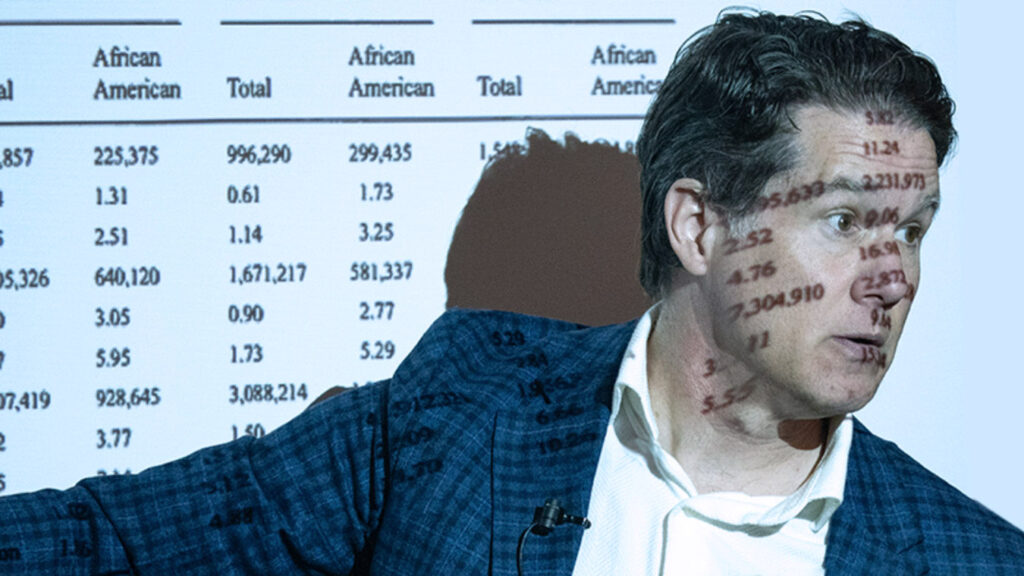
“There’s something about it that changes your fate, and the scope and dimensions of this issue are underappreciated and quite large,” said Schnittker. “One of the first tasks of our book research was to estimate, at the state level and nationally, how many people were either currently in prison or formerly in prison and had a felony record. This is very difficult to catalog, in part because we can count the number of people who are in prison. But the number of people who were formerly in prison is more difficult.”

“We started with the idea that we actually know a fair bit about the folks who are in prison,” he continued. “But once people are released from the prison system, they’re lost to our understanding, and we wanted to focus on this huge part of the equation and figure out what their fate was with respect to health.”
Millions of Americans are incarcerated or were formerly incarcerated and carry felony records. By 2010, he said, about 3% of U.S. adults — and up to 15% of Black men — had direct experience with the criminal justice system, making its health impacts both widespread and deeply unequal.
An unexpected finding of the project was a paradox: For some high-risk individuals, health may temporarily improve during incarceration due to structured environments and access to basic medical care. However, these gains reverse sharply after release. Formerly incarcerated individuals face significantly higher risks of infectious diseases, stress-related conditions, drug overdoses, and overall poor health.
Using advanced methods and natural experiments, including policy changes in Denmark, Schnittker found that incarceration itself causally worsens health, particularly mental health. It more than doubles the risk of mood disorders such as major depression, which can undermine employment, relationships, and long-term stability. “Depression is the leading edge of the incarceration effect,” he said, noting that mental health conditions often play a central role in why formerly incarcerated individuals struggle to reintegrate after their release.
At the same time, a prison record carries severe stigma. Individuals perceive themselves — and are perceived by others — as significantly lower in social standing, even within their own communities. This stigma is particularly strong among African Americans and contributes to lasting economic and social disadvantages.
The health impact is not solely on the individual but ripples throughout his or her family as well. For example, when fathers are incarcerated, mothers face sharply increased risks of major depression, independent of income loss or caregiving burdens. Children are also adversely affected, contributing to intergenerational harm.
Health systems themselves can be negatively affected when substantial numbers of formerly incarcerated individuals enter them and add to local demand for uncompensated care. That can ultimately lead hospitals to cut services, reduce staffing, or diminish access to and quality of care — even for people with no direct connection to incarceration.
Schnittker concluded his remarks by recommending policies focused on effective solutions, including:

LDI Fellows Weigh in on the HBO Max Show, Describing Real Challenges From High Patient Bills to Assaults on Nurses in the ER

Federal Officials Factor in Health Gains to Control Spending, LDI Fellow Says

Former Obama and Trump Advisors Find Some Common Ground at D.C. University of Pennsylvania Event

New York Commissioner Warns University of Pennsylvania Conference That Funding Losses Could Force States to Ration Care and Risk Rising Overdose Deaths

LDI Experts Are Making Postpartum Care Safer With Telehealth, Remote Monitoring, Doulas, and Long-Acting Addiction Care

Researchers Urge Expanding Insurance Coverage with Stronger Environmental Protections to Ease the Biological Toll of Lead and Other Hazards