
Medicare Advantage ‘Working’ for Seniors, but Not for Taxpayers, Experts Say
Penn LDI Panel Cites Costs for Enrollees Alongside Billions in Overpayments and Systemic Gaming
Improving Care for Older Adults
Blog Post
Exercise is medicine for people with Parkinson’s disease. It can improve quality of life and may even slow disease progression. Increasing daily physical activity among people with Parkinson’s disease is important, but effective, low-cost strategies are lacking.
A new, nonrandomized study by LDI Senior Fellow Kimberly Waddell and colleagues found that a remote intervention using game elements shows promise for U.S. veterans with Parkinson’s disease.
The team used behavioral economics principles to increase daily steps among participating veterans. Automatically delivered through a web-based platform, the gaming intervention used loss-framed points and levels to motivate participants to meet their daily step goal.
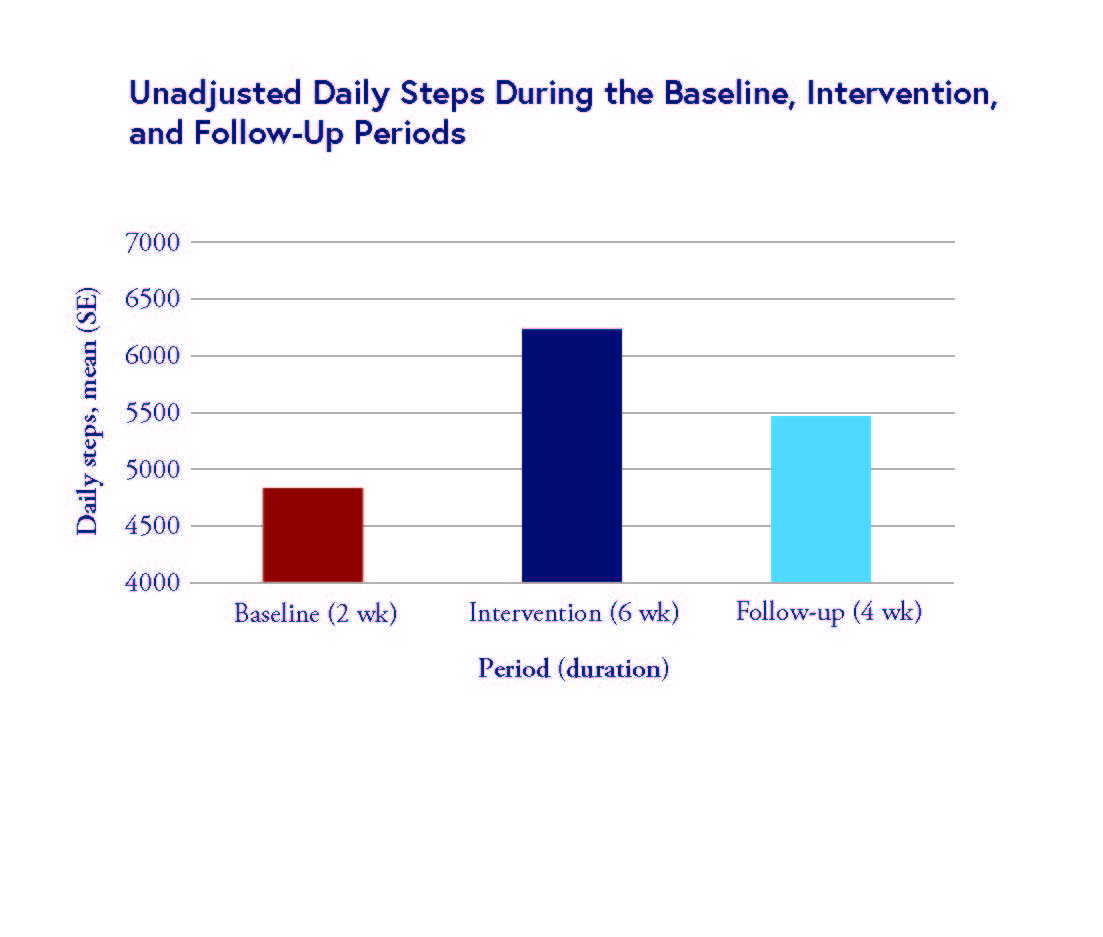
The chart above shows that gamification effectively increased daily steps by 28% during the six-week intervention and by 12% during the four-week follow-up.
Though limited, the findings support the use of gamification as a way to increase physical activity in this group. Furthermore, the automated, remote design holds potential as a way to reduce staffing requirements while eliminating the need for in-person visits.
Waddell writes in the paper that remote, automated behavioral interventions show significant promise for delivering scalable, lower-cost opportunities to increase physical activity in people with Parkinson’s disease.
The article, “Remote, Automated Gamification and Community-Based Physical Activity in Parkinson Disease,” was published in JAMA Neurology on Nov. 3, 2025. Authors include Kimberly Waddell, S. Ryan Greysen, Mitesh S. Patel, Madison S. Smith, Abby Yuen Tsz Lau, Sharon X. Xie, Stephanie Wood, and James F. Morley.

Penn LDI Panel Cites Costs for Enrollees Alongside Billions in Overpayments and Systemic Gaming

New Evidence Undercuts Industry Warnings and Supports the Case To Restore Federal Minimum Staffing Standards

Washington State’s First-in-the-Nation Insurance Plan Begins Payouts in Mid-2026, and Researchers Will Weigh its Effect on Care, Costs, and the Long-Term Care Markets

Issue Brief: Understanding Gaps and Opportunities to Advance Research and Policy

An LDI Fellow Draws on Historic, Paradigm-Shifting Treatments in Depression and Obesity to Consider What Meaningful Breakthroughs in Dementia Care Could Look Like

A Penn LDI Virtual Panel Looks Ahead at New Possibilities