Brief
Prior Authorization Requirements for Proprotein Convertase Subtilisin/Kexin Type 9 Inhibitors Across US Private and Public Payers
Administrative requirements may limit access to treatment

Jalpa A. Doshi, Justin T. Puckett, Michael S. Parmacek, Daniel J. Rader
Circulation: Cardiovascular Quality and Outcomes — January 2018
Key Findings
A comprehensive review of prior authorization (PA) requirements for a new class of expensive cholesterol-lowering drugs known as proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors has found unusually complex and burdensome demands across public and private insurance plans in the United States. These findings raise concerns that current policies may create undue barriers to care even in medically appropriate patients, particularly since requirements were just as stringent for patients with a genetic condition that creates more clear-cut eligibility for PCSK9 inhibitor treatment.
The Question
Are PA requirements for PCSK9 inhibitors serving an appropriate gatekeeping function or creating excessive barriers to treatment? Alirocumab (Praluent®) and evolocumab (Repatha®) were approved by the FDA in 2015 and are thus far the only PCSK9 inhibitors on the market. These novel biologic medications are an innovative option for patients with familial hypercholesterolemia or clinical atherosclerotic cardiovascular disease who require further lowering of LDL cholesterol. Recently completed long-term outcomes trials for both PCSK9 inhibitors have shown significant relative risk reductions in cardiovascular events. In addition, the alirocumab trial reported a lower risk of death overall, with its protective effects being more pronounced in high-risk patients.
Initial estimates placed the number of patients eligible for PCSK9 inhibitors at 9-11 million, with annualized spending projections (depending on uptake assumptions) ranging from $21.4 -$113 billion after accounting for direct medical cost offsets. The fear of a “budget busting” effect should these agents see widespread adoption spurred payers to implement utilization management policies to attenuate the potential economic impact. Early anecdotal reports indicate that the PA process for PCSK9 inhibitors has been particularly challenging for providers, and claims-based studies have reported high rates of rejections of PCSK9 inhibitor prescriptions, with less than half ultimately receiving approval after appeals. Given that target patient populations are at high risk for heart attack or stroke, delays in care related to administrative hurdles could have serious implications.
Using a unique data source, the authors undertook the first detailed analysis of administrative and clinical PA requirements for PCSK9 inhibitors under commercial insurance, health insurance exchanges (HIX), Medicare, and Medicaid, and compared the relative PA burden for PCSK9 inhibitors to that of two other cardiometabolic drugs, namely ezetimibe (Zetia®) and liraglutide (Victoza®), that share key characteristics.
The Findings
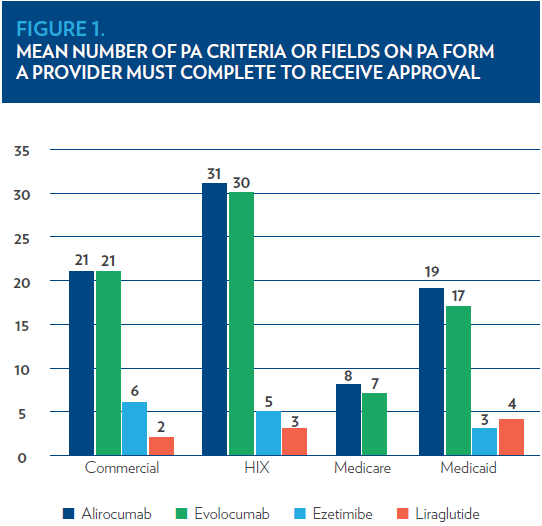
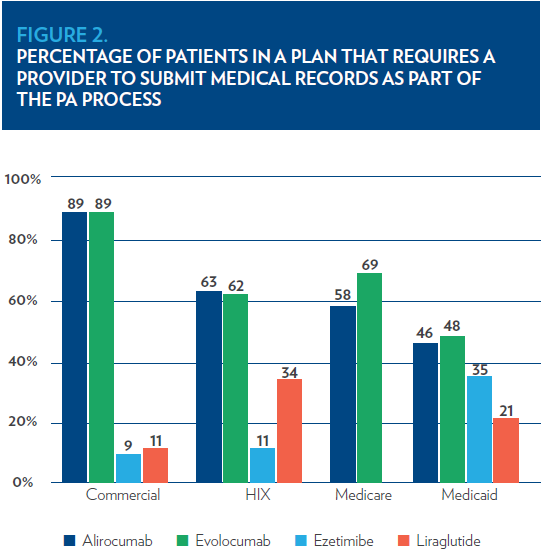
In 2016, between 82% and 97% of individuals were enrolled in plans implementing PA for PCSK9 inhibitors (depending on insurance segment), and one-third to two-thirds of these enrollees faced PAs restricting prescribing of PCSK9 inhibitors to a specialist (e.g., cardiologist). For patients with familial hypercholesterolemia, diagnostic confirmation via genetic testing or meeting minimum clinical scores/criteria was frequently required. PA requirements were more extensive for PCSK9 inhibitors than the other cardiometabolic drugs; forms for PCSK9 inhibitors contained 3 to 11 times the number of PA criteria or fields (Figure 1) and more frequently required the submission of medical records as supporting documentation (Figure 2).
Despite minimal explicit step therapy requirements, most patients (outside of Medicare) were required to try multiple lipid-lowering drugs before receiving PA approval for PCSK9 inhibitors (i.e., implicit step therapy). In addition, there was little consistency regarding which combinations of lipid-lowering medications or dosages payers deemed necessary to fulfill these requirements.
The Implications
These findings offer a rare snapshot of PA burden, which is typically difficult to obtain due to the diverse insurance market in the US and the fact that PA requirements are not necessarily publicly available. The analysis identified five frequent and notable features of PA requirements for PCSK9 inhibitors: 1) more submission requirements for medical record documentation along with PA form, compared to other drugs prescribed by the same types of clinicians; 2) requests for documentation that may be difficult for providers to obtain, particularly if patients have changed physicians over time (e.g., off-treatment cholesterol levels); 3) restriction to specialty prescribers, despite the fact that high cholesterol is often treated in primary care; 4) requirements for genetic testing, which is not standard clinical practice in the US and often not covered by insurance even when required for PA; and 5) step therapy requirements that are not in keeping with clinical guidelines. Collectively, these hurdles may introduce substantial additional out-of-pocket costs for patients (e.g., lab tests, specialist visit copays), which could increase the risk of health disparities among rural and low-income patients and increase the risk that clinically appropriate patients will not receive treatment. In addition, the complexity and variation of requirements across plans also increase the risk of confusion and oversights during PA completion, which may partly explain previous reports of high rejection rates for PCSK9 inhibitor prescriptions.
Given the cost of PCSK9 inhibitors and the number of patients potentially eligible for treatment, payer concerns over the budget impact of these therapies are justified. However, these findings raise the question of whether current PA policies are limiting access to these drugs for even high-risk patients and highlight the relevance of recent efforts to streamline and standardize PA requirements to reduce provider burden while ensuring clinically appropriate use. It remains to be seen how payers will respond to accumulating evidence on PCSK9 inhibitors from long-term cardiovascular outcomes trials, but striking the right balance between access and affordability will be critical to ensuring PCSK9 inhibitors provide maximum value to high-risk patients.
The Study
The researchers conducted an analysis of 2016 formulary coverage and PA data from a large, proprietary database (Decision Resource Group’s Fingertip Formulary) containing information on policies from 3,872 plans across the four major insurance segments (commercial, health insurance exchange, Medicare, Medicaid). These data were linked with enrollment information obtained from Decision Resource Group’s Managed Markets Surveyor-Rx Suite, a second proprietary database containing membership information for insurers in the US. The linked data captured the formulary coverage, tier status, step therapy, and PA requirements for PCSK9 inhibitors for over 95% of Americans (275.3 million lives) who had insurance coverage in 2016.
Key measures included administrative PA criteria (prescriber specialty, number of criteria in PA policy or number of fields on PA form, requirements for medical record submission, reauthorization requirements) and clinical/diagnostic PA criteria (approved conditions, required labs or other tests, required concomitant therapy, step therapy requirements, continuation criteria) for each of the two FDA-approved PCSK9 inhibitors approved at that time (alirocumab [Praluent®] and evolocumab [Repatha®]). Select measures were obtained for two comparator cardiometabolic drugs (ezetimibe [Zetia®] and liraglutide [Victoza®]).
Funding Source
This study was supported by Regeneron and Sanofi. The funding sources had no role in the design and conduct of the study; management, analysis, or interpretation of the data; preparation or approval of the manuscript; or the decision to submit the manuscript for publication.
Lead Author

Jalpa Doshi, PhD is Professor of Medicine at Penn’s Perelman School of Medicine. Her work applies health economics, outcomes research, and policy methods to address issues related to pharmaceutical access, costs, outcomes, and value. In recent years, her research program has particularly focused on specialty drugs for serious, rare, and/or chronic diseases. Dr. Doshi is Director of Value-Based Insurance Design Initiatives at the Center for Health Incentives and Behavioral Economics and Director of the Economic Evaluations Unit of the Center for Evidence-Based Practice at the University of Pennsylvania Health System.