Blog Post
Care Management for Medicaid Patients
Study Finds Insurer-Led Program Did Not Affect Early Costs, Utilization
Five percent of Medicaid enrollees account for nearly 50% of Medicaid spending, making this high-cost group a promising target for care management programs. But a recent study by LDI fellows Arman Oganisian, David Grande, Nandita Mitra, Krisda Chaiyachati, and colleagues found that an insurer-led care management program for high-cost, high-need Medicaid patients did not reduce total costs of care or utilization in the first 12 months after enrollment.
The Community-Based Care Management program (CBCM) was a partnership between a Pennsylvania Medicaid managed care organization (MCO) and health care provider organizations concentrated in North and West Philadelphia. The program paired nurse care managers with community health workers (CHWs) to provide a range of services, from care coordination and medication management, to social needs screening and connections to community resources. The program targeted patients who were in the top 10% of costs for the MCO in the prior year and received care at one of 12 participating primary care sites.
The authors used Medicaid claims data to identify 896 adults who were enrolled in CBCM sometime between January 2016 and December 2017, and compared them to 2,152 similar high-cost patients who were not enrolled in the program. CBCM enrollees and controls were matched on demographics, clinical characteristics, years of continuous Medicaid enrollment, and the month/year of their primary care visit.
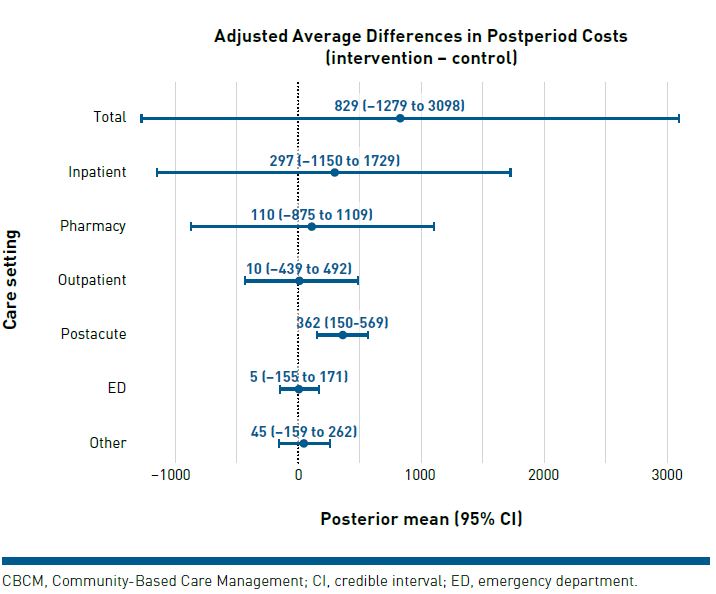
After adjusting for patients’ pre-program costs, the authors found no significant differences in total spending and spending by specific care settings between CBCM enrollees and controls in the subsequent year (Figure 1). CBCM enrollees had 1.55 fewer visits than controls, which was primarily driven by fewer primary care visits. In both groups, total cost among persistent high spenders increased during the study period, while total costs among intermittent high spenders decreased.
Previous studies have shown that CHWs can reduce patient hospitalizations, increase access to care, improve clinical outcomes, and lower costs among high-cost, high-need populations. So what might explain these contradictory findings?
First, how care management programs are implemented can greatly affect cost, utilization, and patient outcomes. Successful programs—such as Individualized Management for Patient-Centered Targets or “IMPaCT,” a Penn CHW program for Medicaid beneficiaries with complex needs—have addressed some of these challenges by developing standardized, evidence-based practices to train CHWs and ensure fidelity to the intervention. In this study, CBCM implementation may have varied across the 12 primary care sites, which were owned and operated by different provider organizations. Each site employed the CHWs, while the MCO employed the nurse care managers.
Second, this study evaluated the first year of the program. The MCO and partnering provider organizations may have corrected early implementation challenges. The true effects of CBCM may not be observed until these challenges have been addressed. Third, since patients were enrolled in CBCM during their primary care visits, the sample does not include high-cost enrollees who missed or delayed care. Programs that can identify and enroll these individuals may observe different outcomes.
This study focused on patients in one insurance plan in an urban area, and did not capture economic benefits of CBCM in subsequent years or noneconomic benefits such as patient satisfaction with care. Because it did not assess clinical outcomes, it cannot say whether the program was cost effective, but it does indicate that the program did not reduce costs. Further research is needed to understand how to structure and implement care management programs to fulfill their promise for high-cost, high-need populations.
The study, “Economic Outcomes of Insurer-Led Care Management for High-Cost Medicaid Patients,” was published in the American Journal of Managed Care on July 13, 2020. Authors include Jordan M. Harrison, PhD, Arman Oganisian, MS, David T. Grande, MD, MPA, Nandita Mitra, PhD, Manik Chhabra, MD, MSHP, and Krisda H. Chaiyachati, MD, MPH, MSHP.