Blog Post
Chart of the Day: Hospital ‘Capture’ Rates for ED Returns
Patients don't stick to one health system for emergency care
A new study in Health Services Research from Penn MSHP alumna Kristin Rising, Penn LDI Adjunct Senior Fellow Brendan Carr, and their colleagues at Jefferson University quantifies something that seems like common sense – patients don’t stick to just one health system for emergency care.
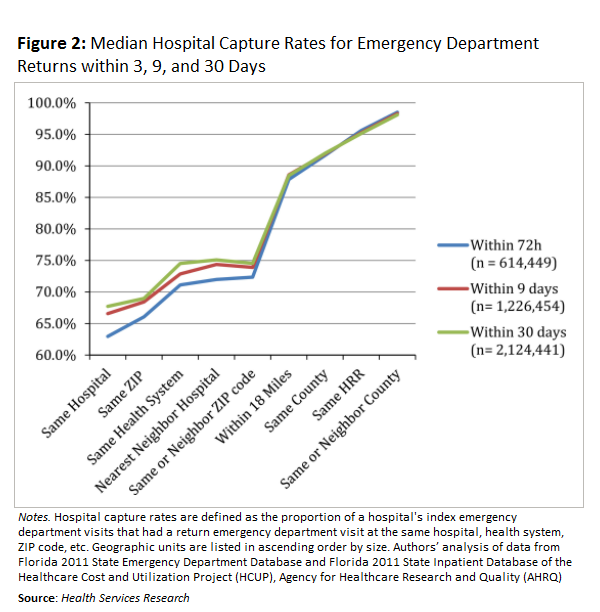
Using data on almost 10 million emergency department (ED) visits in Florida between January 2010 and June 2011, the authors found that almost a third of ED return visits in the month following discharge occur at a different hospital. This number is even higher in the first 48 hours after discharge. The finding confirms prior research, but the study takes one further step: it analyzes where those that do not return to the same hospital go for care, to find the geographic unit of analysis that would ‘capture’ most of the return visits. The authors find that 92 percent of return visits would be captured by analysis at the county level.
This new information has implications for population-based ‘value’ payment structures, where patients are attributed to a single provider or health system. The authors propose that shared accountability across competing health systems, within defined geographic communities, may be an important step on the path to population-based payments and improved outcomes.
The fact that patients jump around between EDs shouldn’t come as a surprise. You don’t have to look further than Philadelphia to see how a person’s health ‘community’ wouldn’t adhere to health system boundaries – within the city there’s a choice of EDs between Jefferson, Temple, Hahneman, and of course Penn. As the authors assert, “regional collaboration across unaffiliated institutions is important for continuity of patient care – safer and more efficient emergency care.”
Read the full study for more on methods and further implications for policy.