Health Care Access & Coverage
Blog Post
MIPS APMs In The Quality Payment Program
Part 3 of a 3-part Health Affairs blog series
[Reposted: Joshua M. Liao and Amol S. Navathe. MIPS APMs In The Quality Payment Program, Health Affairs Blog, October 31, 2018. https://www.healthaffairs.org/do/10.1377/hblog20181030.290056/full/: Copyright ©2018 Health Affairs by Project HOPE – The People-to-People Health Foundation, Inc.]
Launched in 2017 to reward high-value clinicians with upward reimbursement adjustments and penalize low-value clinicians with downward adjustments, the nationwide Medicare Quality Payment Program (QPP) consists of two potential participation tracks: the Merit-based Incentive Payment System (MIPS) and the Advanced Alternative Payment Model (AAPM). In recent posts, we detailed how strong performance in the MIPS track may not lead to the frequently referenced maximum reimbursement increases (for example, ±4 percent in 2017 and ±5 percent in 2018) and implications for clinicians. Instead, actual increases could potentially exceed or fall below those amounts due to how Medicare funds adjustments and how clinicians’ performance relative to others impacts their MIPS scoring.
A related and equally important issue for clinicians is to understand AAPM participation as an alternative that may exempt them from MIPS. An alternative payment model (APM) qualifies as being “advanced” if participating clinicians bear downside financial risk and are measured on their quality performance. For example, clinicians can qualify for the AAPM track by participating in nationwide initiatives such as Bundled Payments for Care Improvement-Advanced (BPCI Advanced) and some options within the Medicare Shared Savings Program Accountable Care Organization (MSSP ACO) program.
However, similar to the MIPS scoring methodology, there are nuances in how clinicians are designated in the MIPS track—either in general MIPS or as a MIPS APM. In particular, under some circumstances, clinicians participating in an APM may remain subject to MIPS as a MIPS APM instead of qualify for the AAPM track. Given its implications on scoring and reimbursement, clinicians should understand this MIPS APM designation.
MIPS APM Designation and Scoring
Clinicians can participate in an APM and fall under a MIPS APM designation in two ways:
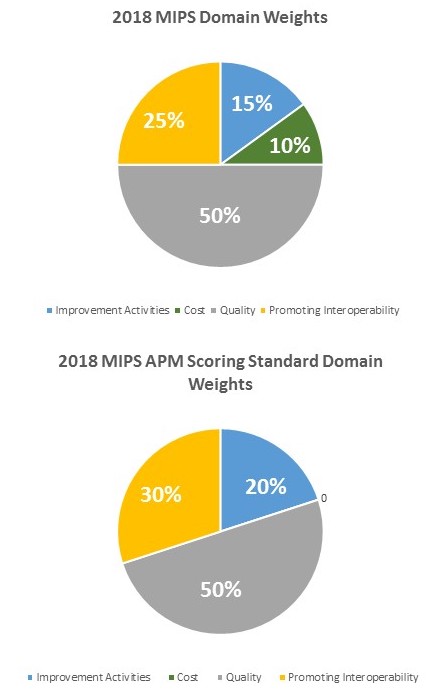
In both cases, the MIPS APM designation is accompanied by a specific scoring methodology—a MIPS APM scoring standard—that differs from the general MIPS scoring standard and is meant to reflect activities already required by the APM (see Exhibit 1).
Source: Medicare’s Quality Payment Program final rules.
- Participating in an AAPM but failing to meet reimbursement or patient thresholds. Beyond accepting downside financial risk, clinicians must also either fully (defined as ³25 percent professional fee payments or ³20 percent patients in 2018) or partially (defined as ³20 percent professional fee payments or ³10 percent patients in 2018) meet reimbursement or patient volume thresholds through an AAPM to be exempted from MIPS. Clinicians who do not meet these thresholds may then be defaulted into MIPS as a MIPS APM. In 2018, Medicare defined five AAPMs for which this could occur: more advanced options (Tracks 2 and 3) in the MSSP ACO program, the Next Generation ACO Model, the Comprehensive End-Stage Renal Disease Care Model, the Comprehensive Primary Care Plus Model, and the Oncology Care Model.
- Choosing to participate in an alternative payment model that is not “advanced” due to lack of downside financial risk. There are situations in which clinicians can choose to participate in an APM that is not advanced by design. A prominent example is Track 1 (or the analogous early “levels,, as currently being proposed in rules changes for 2019) of the MSSP ACO program, in which clinicians and organizations are eligible for shared savings but not liable for shared losses if they fail to lower spending below benchmarks.
MIPS APM clinicians are still evaluated based on the same four general domains as other MIPS clinicians: quality (reporting on clinical quality measures); improvement activities (participation in activities that improve clinical practice); cost (patients’ resource use); and promoting interoperability (demonstration of the ability to use health information technology to engage patients and improve care delivery).
However, assuming sufficient available measures, composite scores for MIPS APM clinicians are calculated using different domain weights. This scoring standard may be preferred because of both its composition and the fact that unlike MIPS domain weights that vary year to year, MIPS APM domain weights are fixed and confer more certainty for clinicians. The latter also pegs the cost domain weight at 0 percent, which allows clinicians to focus on the APM targets (for example, total costs of care in MSSP ACOs, cancer episode treatment costs in the Oncology Care Model) without needing to worry about new MIPS cost measures that emerge (for example, episode-based cost measures). The ability to use quality measures from the APM to fulfill MIPS requirements also reduces reporting burden.
Implications for QPP Participation
The presence of the MIPS APM designation poses implications for clinicians in QPP. Both policy experts and physicians have expressed major concerns about reporting burdens and the ultimate benefit of MIPS. Together with the uncertainty about year-to-year policy changes, such concerns may compel MIPS clinicians to explore other QPP participation alternatives such as upside-only MIPS APMs. This approach may be particularly desirable for clinicians who want to dip their proverbial toes in alternative payment arrangements without absorbing the financial risk needed to qualify for advanced models. However, in these situations, clinicians must also carefully balance their simultaneous potential for financial gains (bonus payments through the APM itself) and losses (downward reimbursement adjustments through MIPS participation).
MIPS APMs may also provide options for clinicians already navigating an evolving APM landscape. For example, lawmakers are currently considering ways to revamp the MSSP ACO program, proposing an overhaul that would require longer participation (five versus three years) and downside financial risk (removal of upside-risk only options). While there is concern that such changes could cause ACOs to drop out of MSSP, this likelihood could be mitigated by the ability to be designated a MIPS APM instead of returning to MIPS. Clinicians could also perceive benefits from a MIPS APM designation if Medicare continues to revise its list of MIPS APMs and consider accommodating new payment arrangements such as BPCI Advanced or physician-focused payment reforms.
Final Thoughts
Clinicians’ QPP participation strategies and decisions will become increasingly complex due to policy evolution in both the MIPS and AAPM tracks. As Medicare modifies programs to accelerate the nationwide shift toward value-based payment, the MIPS APM designation will be an important one for clinicians to consider and policy makers to monitor.