Blog Post
Conflict of Interest Among Public Speakers at FDA Advisory Committees
Prevalent but often undisclosed
Engaging patients, families, and independent experts in policymaking is a laudable goal, but the process of doing so isn’t necessarily straightforward. If efforts to introduce patient and public perspectives also introduce bias, they may do more harm than good. A recent study raises concerns about bias in public engagement, finding that public engagement efforts by the Food and Drug Administration (FDA) may attract speakers with significant conflicts of interest (COI), which are frequently undisclosed.
In JAMA Internal Medicine, Matthew McCoy, Genevieve Kanter, and colleagues raise concerns that FDA public engagement is rife with conflicts of interest. Previous work found that a significant portion of speakers at the FDA Oncologic Drugs Advisory Committee have disclosed and undisclosed conflicts of interests, and public feedback the FDA receives at these committee meetings is overwhelmingly in favor of drug approval. McCoy and colleagues follow up with an investigation of speakers at the FDA Anesthetic and Analgesic Drug Products Advisory Committee (AADPAC), which advises the FDA on therapies used in anesthesiology and pain management, including opioids.
AADPAC is one of 33 FDA advisory committees, which cover topics ranging from cardiovascular and renal drugs to oncologic drugs. Ideally, open committee meetings offer an opportunity for researchers and interested patients to present their views on available treatments, devices, and issues of public health.
The authors reviewed meeting transcripts of AADPAC meetings from 2009 to 2017 and identified 112 speaking appearances made by 91 individuals. Twenty-two of the 112 speakers disclosed a COI, such as reimbursement for travel related to attending the meeting. The authors independently identified undisclosed conflicts of interest that predated the committee meeting for six speakers. In addition, they identified 15 speakers who had undisclosed financial associations with the sponsor of the drug under review but for whom it could not be determined whether the financial association originated before or after the meeting in question. Put another way, at least a quarter of speakers had a conflict of interest, a fifth of which were not disclosed to the committee.
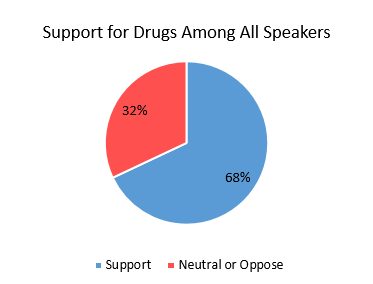
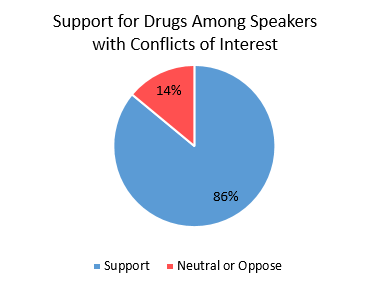
Overall, 67.9% of speakers supported drug approvals. Support for drug approval was significantly higher (86%) among speakers with prior conflicts of interest. Using a logistic regression, McCoy and colleagues estimate that speakers with a disclosed COI are six times more likely to voice support for drug approval than speakers with none.
The JAMA Internal Medicine letter is part of a relatively new line of health policy research that focuses on the context in which decisions regarding funding of biomedical research and the coverage of services are made. Recent work has begun to flesh out the scale of COIs in the health care system, leading many observers to raise alarms that COIs are commonplace, financially substantial, and poorly understood in biomedical research, public policy, and clinical care.
For example, patient advocacy organizations—which frequently lobby for federal funding of biomedical research and expanded coverage of expensive drugs—are coming under increased scrutiny. In 2017, McCoy, Emanuel, and colleagues investigated the financing of 104 patient advocacy organizations. They found that while 88% published a list of donors, only 5% disclosed the exact size of donations. The authors also found that at least 83% of patient advocacy organizations received funding from drug, device, or biotechnology companies, and at least 39% had a current or former industry executive on governing boards. Only 12% of advocacy groups had published policies to manage COIs.
A word of caution: conflicts of interest do not automatically indicate bias or harm. However, conceptual confusion regarding the nature, function, and scope of conflicts of interest in health policy remains widespread. It is worthwhile to consider a simple set of questions: what is a conflict of interest? And how much should we care about them?
All professionals have primary and secondary interests. In medicine, a physician’s primary interest is to improve the wellness of patients through care. In research, the researcher’s primary interest is to produce generalizable knowledge. Professionals also have secondary interests, such as gaining recognition in the field and accumulating wealth. COIs arise when professional judgment concerning a primary interest is at risk of being biased by a secondary interest. COIs do not require direct harm: the simple presence of secondary interest that could bias judgment is required for there to be a COI. Thus, the notion of a “potential” conflict of interest is a conceptual misnomer.
Not all COIs are created equal. The severity of a COI is judged based on the likelihood of bias and the magnitude of possible harm. Therefore, the scale of financial interest is important: the greater financial interest, the greater the likelihood of bias. The severity of a COI may trigger policies to manage or prohibit it. However, it is impossible to manage or assess COIs in health care when researchers simply don’t know the scale of the problem.