Blog Post
Does Collective Bargaining by Physicians Hurt Consumers?
Evidence From a Case of Collusion in Chile
Prices for health care services are a function of negotiations between insurers and providers—and both sides are always trying to gain advantages. In the U.S., providers have tried to increase their leverage over insurers through consolidation—including hospital mergers, vertical integration of hospitals and physician practices, and agglomeration of physician practices into larger multi-specialty groups. But even if doctors and hospitals do not merge, they might still improve their position through collective bargaining. So, what happens when providers bypass mergers and acquisitions in favor of banding together as independent practices? A recent economic case study in Chile, published in RAND Journal of Economics, shows that prices can increase dramatically, with serious consequences for patients.
In their analysis, LDI Senior Fellow Juan Pablo Atal and Jorge Alé-Chilet study the experience of a trade association of gynecologists in Chillán, Chile (population 175,000).
Chile’s health care system includes parallel public and private insurance. While public insurance uses a fee schedule, private rates are negotiated independently. For years, gynecologists in Chillán believed private rates were too low. So, in 2011, 26 out of 29 gynecologists in the city formed the Gynecologists’ Association of Ñuble. The next year, association members simultaneously canceled their contracts with private insurers, set a new minimum fee for office visits, and named a single representative for all future negotiations. The arrangement did not last long. In 2013, the government investigated the association for anti-trust offenses and shut it down in 2016.
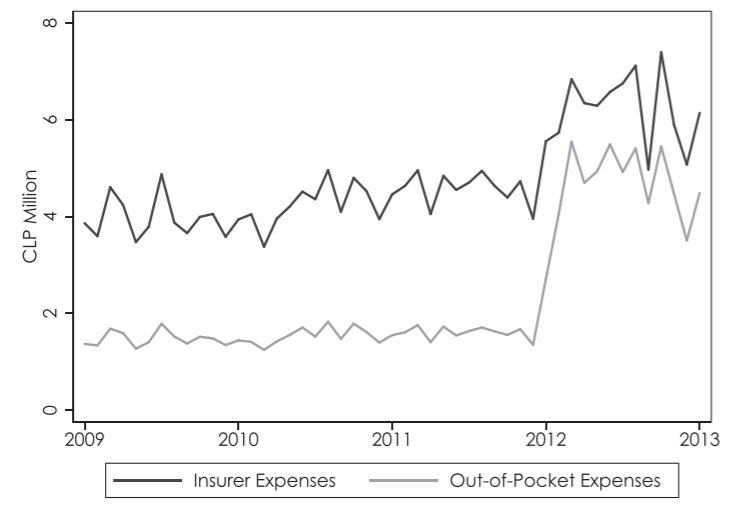
As shown in the figure below, the effect on office visit prices, consumer out-of-pocket expenditures, and provider revenue were large and immediate. Prices for office visits rose by 80%, and patient out-of-pocket costs doubled as coinsurance rates also increased. Consequently, provider profits more than quadrupled. Notably, none of these outcomes changed for gynecologists in neighboring areas, suggesting that the formation of the association drove the changes.
Interestingly, part of why the association of gynecologists succeeded is that providers were correct in their view that private rates were low relative to a competitive market. When the authors modeled local demand, they found that the new prices were in line with what a competitive market would produce: the minimum price set by the new association was close to the equilibrium market price and did not generate monopolistic profits. This finding also helps the authors explain why the incentives for staying in the association were strong. Put another way, gynecologists in Chillán had little bargaining power initially, and the success of their collective negotiations was partially driven by having such a low baseline.
That does not imply there were no harms from the collusion among providers. The widespread breakdown of negotiations between providers and insurers resulted in a substantial cost shift to consumers, who ended up facing higher coinsurance rates on higher prices.
This case of collusion by providers provides some insights into the American context, in large part because it mirrors several similar cases of coordinated contract cancellation under investigation by the Federal Trade Commission (FTC). Some observers suggest allowing small providers to negotiate collectively may be useful in cases where insurers have most of the bargaining power, but in this case, allowing for more collective bargaining shifted costs on to consumers, in addition to private insurers.
This study also has implications for the future of value-based payment. Both the Department of Justice and FTC have allowed joint negotiations with payers when providers are part of Accountable Care Organizations (ACOs). These waivers are controversial, as they raise concerns about increasing provider leverage over insurers and self-referrals by providers. This case suggests that as ACOs are increasingly associated with provider consolidation, policymakers will have to consider possible unintended consequences for consumers when independent providers are allowed to negotiate as one.

The study, Trade Associations and Collusion Among Many Agents: Evidence from Physicians, was published in the November 2020 issue of the RAND Journal of Economics. The authors include Jorge Alé‐Chilet and Juan Pablo Atal.