
U.S. Hospital Nurse Job Conditions Worsen After COVID, and Turnover Continues
Chart of the Day: National Study Shows Worse Nurse Job Satisfaction and Perceived Lower Care Quality as Staffing Shortages Persist Post-Pandemic
In Their Own Words
Warning: Spoilers for the Pitt S2 ahead. This file has been updated with new material.
LDI Fellows use The Pitt‘s second season to show how fictional storylines often mirror real-world challenges—from a violent assault on an ER nurse to a hospice patient whose end-of-life preferences shift amid great pain, and a near-miss caused by a generative AI charting error. While The Pitt is fiction, the policy implications are very real.
Hear from eight LDI experts below. The latest installment was published April 16, 2025.

In Episode 6, Harlow Graham, a deaf patient, communicates via American Sign Language (ASL) with an in-person interpreter, until the interpreter is called away. The care team, with limited ASL proficiency, cannot capture her full history. A Video Relay Interpreter (VRI) is brought to Harlow but it runs into connection issues. A new in-person interpreter arrives to Harlow’s relief, as she dislikes using the VRI.

K. Jane Muir, PhD, APRN: Patients who experience communication barriers are more likely to have repeat emergency department visits, and evidence suggests that it is often due to poor quality care factors, including inadequate access to high-quality language services such as interpreters. Despite regulations in place requiring that hospitals receiving federal funds provide language access and communication services for patients, the quality and availability of interpreters vary across U.S. hospitals. When clinicians are overextended, constrained, and working with faulty technology, barriers to high-quality communication are exacerbated. One evidence-based strategy is to invest in the clinician work environment to avoid medical overuse, care delays, and unnecessary hospital admissions for patients experiencing communication barriers. On the frontlines of care, nurses who work in hospitals with a manageable workload and supportive managers who address their concerns about issues with language access services report more favorable outcomes for patients experiencing communication barriers.
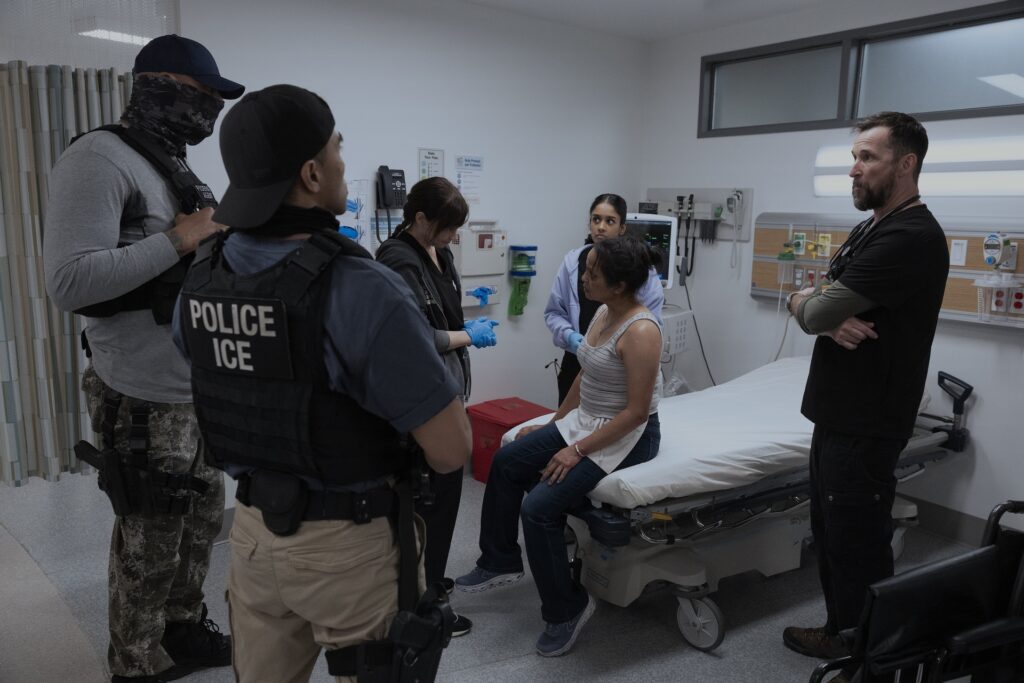
Episode 11 features a harrowing storyline where Immigrations and Customs Enforcement (ICE) Agents enter the emergency room with a detainee that has been injured during an immigration raid. The presence of armed, masked ICE agents triggers panic amongst both patients and staff, causing some to leave, fearing for their safety.

Diana Montoya-Williams, MD, MSHP: This episode highlights the conflict between aggressive immigration enforcement and medical care. Nurse Dana Evans accurately highlights the Emergency Medical Treatment and Labor Act, a federal law passed in 1986 that requires hospitals that accept Medicare to treat patients regardless of ability to pay, insurance status or immigration status. Despite this law, the episode clearly captures the “chilling effect” of intensified immigration enforcement on health care use. A large body of research shows people may delay or avoid seeking care they are legally entitled to because they fear contact with immigration authorities or jeopardizing their path to legal status. The episode correctly shows that this fear does not just affect patients who are undocumented, but many in the community with legal statuses, as even staff members with active legal status chose to leave work in the episode that day out of fear. As Dr. Robby highlights, the irony of not seeking preventative or early emergency care is not that the care is unnecessary, but rather that patients then present later in more acute stages with potentially devastating consequences to themselves and higher costs.

In Episode 2, Orlando Diaz is hospitalized with life-threatening diabetic ketoacidosis after he lost his health insurance and began rationing his insulin. Meanwhile, his family earns too much to get on Medicaid. Even though hospital officials make several efforts to lower care costs, he leaves the hospital against medical advice because he cannot afford even discounted care on top of $100,000 in existing medical debt.

Meredith Doherty, PhD, LCSW: Mr. Diaz is one of the 26 million Americans who lack basic health insurance, the vast majority of whom (73.7%) are working adults whose employers do not provide affordable coverage. Nearly 2 million uninsured workers have diabetes, a chronic illness that can be managed effectively with common treatments, like insulin. Without health insurance, though, many people with diabetes go untreated despite the availability of safe and effective treatment. Financial toxicity—or the financial issues that result from high out-of-pocket medical expenses—is linked to worsened outcomes for cancer patients, which is a focus of my research. Many cancer patients experiencing financial toxicity are uninsured or underinsured.
As seen in this episode, untreated diabetes can quickly snowball into catastrophic health conditions that require critical, emergent health care needs. The sad irony, and frankly the most frustrating aspect for me, as a scientist and advocate, is that the overall cost to society of untreated diabetes and other chronic health conditions is many times greater than that of providing universal access to health insurance and routine care. I am currently the lead investigator on a trial which pairs a financial navigation program with guaranteed monthly income and evaluates its impact on cancer-related financial hardship for patients with low incomes, and I have also investigated how to improve patient access to financial assistance programs.

Episode 4 shows an ER strained beyond capacity as a nearby hospital closure triggers a surge of patients, making staffers to treat nonstop emergencies with little time and few resources. Throughout the series, patient care in the ER often occurs in hallway beds due to limited beds, underscoring a frequent theme of ER overcrowding in the second season.

Austin Kilaru MD, MSHP: Our society takes for granted that when we get sick, we can go to an emergency room and receive immediate attention. But that is often not true. You may have to wait hours to receive care, even if you are truly sick. Why? It is not because ERs, and their dedicated staff, are dysfunctional. In fact, physicians and nurses pull off the impossible every day, helping as many patients as they can. The reason is that the ED has to keep patients that need to be admitted but have no hospital bed to go to. Because patients cannot leave the ED, the lines then spill out the front door. And patients have worse outcomes. If we ask why again, there are deeper reasons — all of which demand that we take action.
Our payment system demands that hospitals keep all their beds full, to make enough money to keep the lights on. Our inability to keep people healthy — through strong primary care, population health, and behavioral health services — fuels the demand for ED and hospital services. And our inability to send patients from the hospital back to their homes or nursing facilities further clogs the system. On top of all of this, the misunderstanding of this problem among health care leaders, along with the lack of good quality measures, aggravates the underlying challenges.
The obvious response — build more hospital beds — will not work without taking other actions in parallel. Building beds increases costs, which raises pressure on hospitals to make more money, which leads to more high revenue procedural and elective care, which attracts more patients that fill the new beds. So — we circle back to the same place but now spend even more money. It is important to note that while some hospitals, often large academic health systems, are overwhelmed, other hospitals struggle to find enough patients to stay open.
We need to do three things. First, pay hospitals in a new way that does not force them to do more but instead keep beds open. Second, create public quality measures that affect hospital accreditation and payment, forcing leaders to act. And third, strengthen our outpatient systems to not only keep people healthy but deliver timely care when people do get sick — new alternatives to EDs and hospitals. These solutions are not easy, but as seen in The Pitt, we have no other choice.

In Episode 11, Dr. McKay and the street medicine team treated Kiki, an unhoused person who uses intravenous drugs. Kiki asks for Dr. McKay to meet her in the park for an issue with a wound from xylazine use, which is beginning to smell. Kiki admits to using “tranq,” xylazine’s common name. Dr. McKay and a medical student clean the wound with saline and give Kiki antibiotics and supplies to treat the wound on her own.

Eleanor Turi, PhD, RN: From a policy perspective, this episode underscores the critical role of delivering wound care outside of the traditional medical system. Street medicine is a health delivery model that brings direct medical care to unsheltered people experiencing homelessness. At the state level, policymakers can strengthen street medicine organizations by supporting implementation of new Medicaid street medicine billing codes, enabling teams to bill for their services. Financial viability may improve by including nurses as eligible providers, my work suggests. Also key are expanding the range of reimbursable services, simplifying billing processes, increasing reimbursement rates, and supporting bulk funding mechanisms. At the local level, policymakers should continue to support, not reduce or restrict, harm reduction services like street medicine teams and syringe services programs, which are essential to maintaining accessible wound care for people who use drugs. Finally, payers can support innovation by reimbursing telehealth models that extend specialty wound care into community settings; I am currently testing one such tele-wound care consultation model through the Penn Nursing Innovation Accelerator.
Read more about what The Pitt got right and wrong about xylazine wounds on Eleanor’s Substack.

In Episode 10, Roxie, 42, a hospice patient with advanced lung cancer, debates whether to return home to die as her husband wishes. Dr. Robby asserts supporting her choices is the best thing they can do for her. She ends up dying in the hospital with her family by her side.

Katie Auriemma, MD, MSHP: Dying at home is often touted as a central part of a “good death”. Dying at home is cited as the majority preference of Americans. Hospital deaths, particularly for patients enrolled in home hospice, are often considered a system failure. However, preferences for end-of-life care are not always stable, and the reality of caring for someone at the end of life in the home setting, even with supportive services, can be incredibly challenging for patients and families. The importance of eliciting and honoring shifting preferences over time or with changes in health status is central to the provision of goal-concordant care. On a system level, we need better methods to identify and measure delivery of goal-concordant care so that “place of death” is not the only marker of a “good death.”

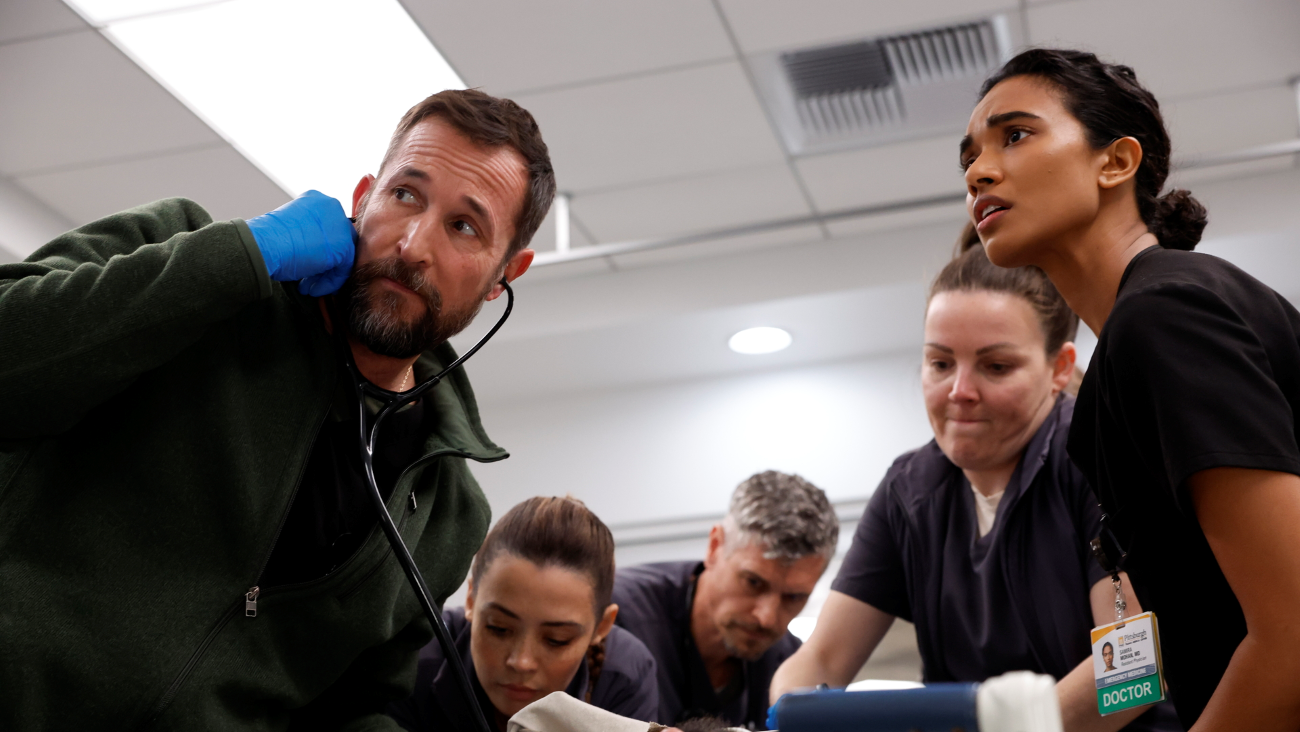
In Episode 6, a generative AI charting tool, championed by Dr. Al-Hashimi, makes a critical mistake by hallucinating a patient’s history, including a false appendicitis record and incorrect medications, nearly causing a dangerous medical error. This highlights risks of over-dependence on AI and the need for human oversight.

Eric Bressman, MD, MSHP: Though the scene is fictional, the risks it highlights are real. Generative AI documentation tools can hallucinate, inventing details or misstating key facts about a patient’s history. Likewise, automation bias–the tendency to over-rely on the information that AI generates–is a well-documented challenge. In medicine, these kinds of errors can propagate from a charting error into a genuine patient safety problem. The solution is both simple and complex. At the local level, we need to create the conditions for more consistent and reliable review of AI-generated information, both by human providers and, potentially, secondary AI systems designed to flag errors. More broadly, as adoption accelerates, the larger challenge is building rules for clinical AI that emphasize validation, transparency, and accountability before convenience outruns patient safety.
In Episode 11, Emma checks on a sleeping patient who was taken to the hospital for combative behavior and intoxication. The patient wakes up, confused and still combative, and places Emma in a chokehold. She cannot call for help because the room’s door is closed.

Karen Lasater, PhD, RN: Nurses in emergency departments (ED) are assaulted on the job more than nearly any other professional in any industry. In the absence of national standards to prevent workplace violence against health care workers, legislative action is progressing piecemeal across states, or at the discretion of hospital administration, making protection for health care workers uneven. Nurse understaffing in hospitals has been associated with greater incidence of workplace violence and can be addressed through policy mandates to ensure safe care environments for clinicians and patients alike. Understaffing of nurses in inpatient units contributes to bottlenecks in the ED, with patients boarding in hallway beds and leaving before care is finished due to frustrating care delays in the chaotic and high-stress environment. For these reasons, ED clinicians endorse safe nurse staffing standards (among others) as a workplace violence prevention strategy.
Chart of the Day: National Study Shows Worse Nurse Job Satisfaction and Perceived Lower Care Quality as Staffing Shortages Persist Post-Pandemic

Chart of the Day: Remote Intervention with Gaming Elements Shows Promise, LDI Expert Finds

Cited for Driving Changes in Early Pregnancy Loss Care Guidelines

Penn Researcher Says Mental Illness, Chronic Disease Risks Surge After Release

Federal Officials Factor in Health Gains to Control Spending, LDI Fellow Says

Former Obama and Trump Advisors Find Some Common Ground at D.C. University of Pennsylvania Event