
Incarceration as Social Determinant of Health
Penn Researcher Says Mental Illness, Chronic Disease Risks Surge After Release
Blog Post

Tens of billions of dollars in federal, state, and municipal assistance remain unclaimed each year because people who are eligible do not apply for programs that provide tax relief, food, help with energy bills, and other programs that address health-related social needs.
LDI Senior Fellows Austin Kilaru, Raina Merchant, Anish Agarwal, and colleagues tested ways to motivate patients in the emergency department to contact a benefits navigator and explore the programs they might be eligible for. Providing an informational flyer in the emergency department did not motivate action, the researchers found. However, one-quarter of patients who received the flyer along with follow-up text messages in the two weeks after their visits reached out to the benefits navigator, and 18% applied to at least one program.
With support from a Dean’s Innovation Award and Accelerate Health Equity, a Philadelphia-wide initiative to address underlying causes of health disparities, the researchers conducted a randomized trial of 160 patients in two city emergency departments. All participants were informed about benefits for which they might qualify and received a paper flyer that included a phone number to reach benefits navigators from a community partner. The 79 participants in the intervention group also received a series of automated text messages at regular intervals after discharge.
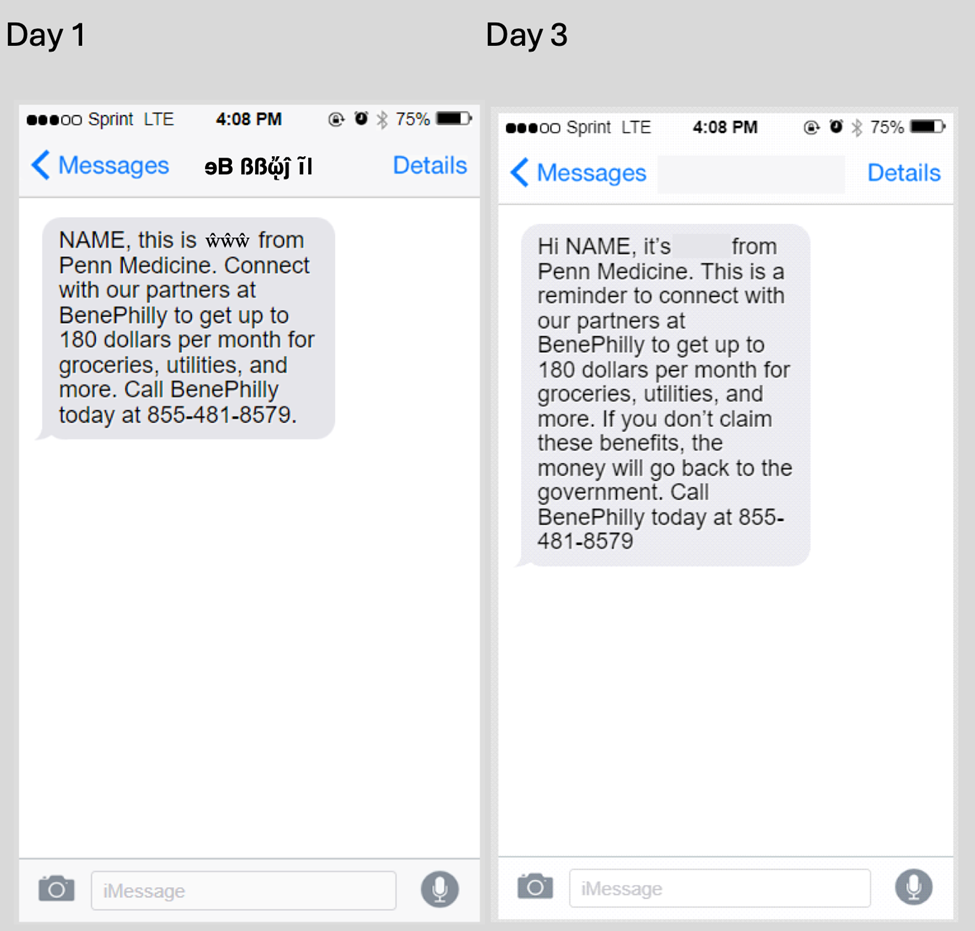
The messages included prompts to call and incorporated behavioral economics strategies such as loss aversion, where the fear of losing outweighs the prospect of winning, and psychological ownership, where the benefit can be seen as rightfully theirs. See Figure 1 for examples of messages sent on day one and three.
After 14 days, no participants in the control group contacted a benefits navigator. In contrast, 25% of participants in the intervention group did, and 14% submitted an application for public benefits. At 30 days, that number rose to 18%.
As for timing, most calls to benefit navigators occurred within the first three days after discharge, with peaks on days when text messages were sent (days one and three). Only two calls occurred after day seven during the 14-day intervention period.
Access to benefits is strongly linked to improved health outcomes, particularly for low-income populations who rely on the health care safety net provided by emergency departments. They represent viable settings for engaging patients about their eligibility for public benefits, Kilaru and colleagues have shown.
Emergency departments typically discharge patients with paperwork about their care. This study shows that text messaging after discharge improves engagement compared with standard paper-based approaches.
The study, “Linkage of Emergency Department Patients With Public Benefits Navigators via Text Messages: A Randomized Clinical Trial” was published February 6, 2026 in JAMA Health Forum. Authors include Austin S. Kilaru, Aliza Haider, Joseph Harrison, Erica L. Dixon, Lauren Southwick, Melissa Berkowitz, Charles Rareshide, Conor Carroll, Clayton Kaledin, Grace McDermott, Michael Mehta, Alisa J. Stephens Shields, Wendy De La Rosa, Anish K. Agarwal, and Raina M. Merchant.

Penn Researcher Says Mental Illness, Chronic Disease Risks Surge After Release

LDI Experts Are Making Postpartum Care Safer With Telehealth, Remote Monitoring, Doulas, and Long-Acting Addiction Care

Researchers Urge Expanding Insurance Coverage with Stronger Environmental Protections to Ease the Biological Toll of Lead and Other Hazards

Faster Access to Stable Housing May Improve Health for Vulnerable Veterans, LDI Fellows’ Study Finds

Former Philadelphia Health Commissioner Releases Policy Brief as City Council Weighs Stronger Tenant Protections

First Rural Health Grants May Not Go to Areas With the Greatest Needs, LDI Experts Find