Key Findings Local police officers and other external law enforcement officers are ubiquitous in emergency departments (EDs) across the country. But the job of law enforcement to protect public safety can sometimes conflict with clinicians’ dedication to patient care while putting patient privacy, autonomy, and trust at risk. This brief reviews published work examining ambiguities around the role of law enforcement in EDs.
Consider the following questions, all of which involve situations that potentially further public safety but also may come at the cost of patient privacy:1
What should clinicians do when a police officer asks them to draw blood from an unconscious ED patient for law enforcement purposes?
Under what circumstances should an officer be allowed in patient care areas, where they could overhear protected health information?
When can officers question seriously injured patients?
When is disclosure of personal health information to law enforcement officers required, optional, or unethical without patient consent?
Should ED staff allow officers access to a patient’s belongings?
To help answer these questions, hospitals and their staff need clear institutional and professional policies. But this such policies are frequently lacking—and the policies that do exist can prioritize law enforcement goals over patient care.2 Clinicians are often left to make case-by-case decisions at the bedside with little guidance.
To help clarify, inform, and improve interactions between law enforcement and clinicians, we have drafted this brief to review the reasons for the prevalent law enforcement presence in the ED; describe related challenges; present stakeholder perspectives; and recommend ways to implement policy in this critical area. To address the perspectives of clinicians, we use data from emergency physicians and trauma surgeons, since the existing body of research focuses on these groups.
The Many Paths that Lead Officers to the ED
Police officers are a frequent presence in EDs. They accompany individuals in custody, investigate crimes, and respond to calls from hospital staff and patients. In one urban ED, an officer was present 31% of the time, according to an observational study.3 A third of emergency medicine physicians participating in a national survey reported that at least one officer was present in their ED daily.4 Meanwhile approximately 2 in 10 trauma surgeons reported law enforcement officers were present in trauma bays daily, and 8 in 10 reported they were present weekly.5
How do these officers end up in the ED?:
Local policies can create pathways for police presence in the ED. “Scoop and run” policies in Philadelphia, Sacramento, Detroit, and elsewhere, enable officers to arrive at the site of a serious injury before medical responders and may transport injured patients directly to the ED for trauma care.6 Officers often accompany people who are incarcerated or under arrest to the ED for necessary medical care. The most common reasons for law enforcement presence include accompanying a patient under arrest; accompanying a patient who was agitated, altered, or intoxicated; and accompanying a patient who was incarcerated or jailed.7
Health systems may call external law enforcement into the ED. This may occur if mandatory reporters suspect abuse or maltreatment of children or vulnerable adults or where compelled by state policy to report, for example, any injuries caused by violence. Hospital staff also may call law enforcement to respond to safety and security threats, an especially salient reason as rates of violence reported by ED physicians and nurses have increased recently.8
Police officers may enter the ED as part of day-to-day professional practice. More than three-fourths of emergency physicians reported that they had seen police officers in the ED questioning patients as witnesses to, or a suspect of, a crime; nearly three-quarters of trauma surgeons reported that they had observed officers collecting evidence from patients.9
Legal Ambiguities and Ethical Concerns
Patient Rights, Public Safety
The legal ambiguity of many police officer–clinician interactions poses a risk to patient rights, including privacy and autonomy, and may conflict with bioethical principles of beneficence (doing good for patients), nonmaleficence (avoiding harm to patients), and justice (treating patients fairly).
In one example of such conflict, an ED nurse in Utah was arrested when she refused an officer’s request to draw blood from an unconscious patient. In response to public outrage, the state legislature passed a bill limiting the circumstances when police can request blood samples, and the hospital system that employed the nurse banned law enforcement officers from patient care areas.10
Such complex and sensitive interactions can rely on nuances of municipal, state, and federal law, including intricacies of constitutional criminal procedure, that clinicians would not be expected to understand at the bedside of a patient in the ED. Similarly, the law enforcement officers in more than 16,000 local agencies across the country may not understand the boundaries of their authority within specific health care settings.
Clear hospital policies and professional guidelines are needed, but few have been developed and implemented at the hospital level. Only about 21% of trauma surgeons reported that their institutions had a policy to guide police interactions with trauma patients, while 73% identified a need for one.11 Similarly, only 13% of emergency physicians said that they were aware of a policy or guideline to inform officers’ interactions with ED patients.12 Notably, relying on federal jurisprudence skews outcomes towards police by prioritizing public safety, and thus away from patient privacy in ways that may challenge the notion of EDs as “places of healing”.13 More guidance, most specifically to protect patients’ rights, is needed.
Existing Guidelines and Resources
Some professional guidelines, including from the American College of Emergency Physicians (ACEP)14 and the Washington State Hospital Association (WSHA)15, address one piece of the puzzle: the release of personal health information to police officers. The ACEP recommends that clinicians release such information only (1) when the patient consents, (2) when reporting is mandated, or (3) when an officer produces a subpoena or other court order; the WSHA makes similar recommendations. But the ACEP guidelines also advise physicians to use their judgment and discretion in sharing information with law enforcement, emphasizing clinicians’ “fundamental professional responsibility to protect the confidentiality of their patients’ personal health information.”
Several other resources have been developed recently to help clinicians understand and navigate this complex terrain. These include:
An ethical framework to guide interactions with law enforcement in trauma care settings from The American Association for the Surgery of Trauma’s Injury Prevention (AASTIP). The framework suggests that bioethical principles are “a universal common ground” that can help hospitals, law enforcement, and communities develop fair and transparent policies.16 AASTIP gives examples of how this framework can be applied using case scenarios.
A toolkit from a multidisciplinary working group from Georgetown University that provides clinicians with practical guidance on how they can interact with law enforcement officers to safeguard patient rights and to promote safety.17 It includes advice on how to advocate for institutional policy changes within a hospital or health care system.
Clinicians’ Reactions
An Emphasis on Safety
Clinicians perceive law enforcement presence as being more helpful to public safety and clinical care than to patients themselves. Surveys showed that only 38% of emergency physicians18 and 26% of trauma surgeons19 perceived the presence of police as helpful to patients; however, only a minority of the emergency physicians (32%) and trauma surgeons (21%) reported that police presence has a more negative than positive impact on the doctor-patient relationship.
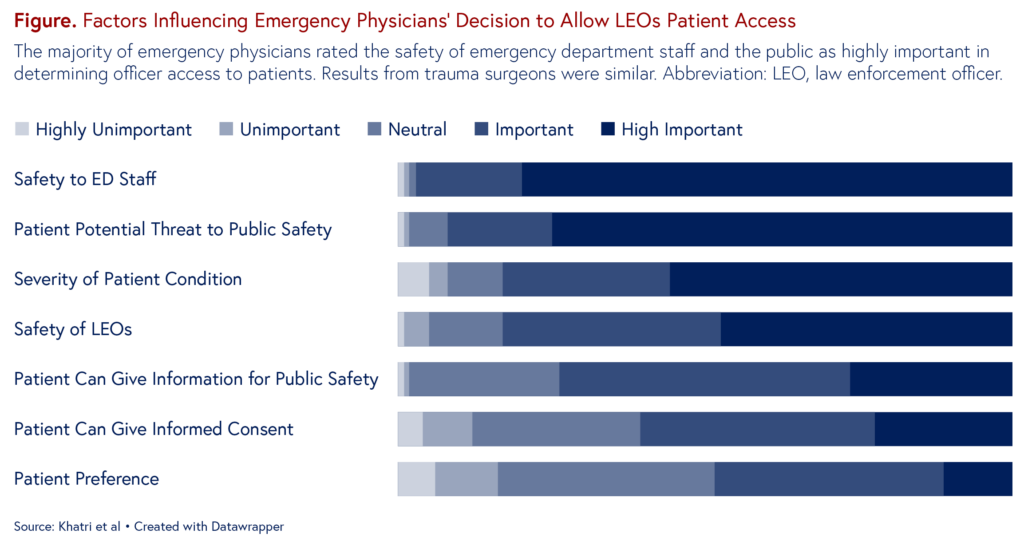
When deciding whether to allow officers access to their patients, both groups cited safety factors and the severity of the patient’s conditions as highly important factors. Patients’ preferences and ability to consent to the interaction were least commonly considered highly important (Figure).
The majority of emergency physicians rated the safety of emergency department staff and the public as highly important in determining officer access to patients. Results from trauma surgeons were similar. Abbreviation: LEO, law enforcement officer.
Although clinicians clearly prioritize safety in interactions with police officers, it is unclear whether the presence of police actually improves safety, given the limited research in this area. A recent narrative review pointed out that increased police presence increased hospital staff perceptions of safety,20 but police presence has not been shown to actually reduce violent incidents in the ED. The authors noted that workplace violence remains widespread even in the face of increasing police and security presence in hospital EDs, and they pointed to promising non-law enforcement strategies such as de-escalation and conflict resolution.
Patient Perspectives
Legal Support, Institutional Racism
Police in the ED can affect patients directly through their interactions, as well as indirectly by undermining trust between patients and clinicians.21 Because communities of color and poorer communities are disproportionately affected by both violent crime and over-policing, the presence of police in the ED must also be considered in the context of institutional and structural racism. Black patients are more frequently subject to “assumed criminality” than White patients,22 a fact that has troubling implications for their interactions with police officers. These interactions may be perceived as threatening and result in fear activation. Findings of a study involving formerly incarcerated Black men suggested that negative interactions with police can have long-term negative consequences, including higher rates of depression.23
In studies from an urban trauma center, Black patients reported that police presence was beneficial when it led to increased support and information after injury,24 but questioning by officers felt stressful and disrespectful.25 Negative interactions with police officers during injury recovery resulted in feelings of anger, helplessness, suicidality, and dehumanization. The Black patients also reported experiencing difficulties accessing victims’ services and other challenges related to the legal system that may further the impression that officers are not in the ED to help patients.
Policy Recommendations
A Call for Guidance
Balancing public safety and patient-centered care should be the full responsibility of individual clinicians and officers in the ED. Hospitals and health systems need to create concrete policies that guide these interactions. To build guidelines that encompass many perspectives, a city’s public health department could convene the area’s hospitals, health systems, and other stakeholders to craft policy together. Important areas to cover include:
Specific law enforcement activities in the ED, including information sharing with officers, information gathering for officers, the security of patient property, the use of physical and chemical restraints, and patient visitation. The Georgetown working group toolkit outlines these activities.
Shared input from the full spectrum of stakeholders, including police officers, clinicians, and patients, to adequately address public safety concerns within the boundaries of appropriate, ethical patient care. A standing committee that includes officers, clinicians, nurses, lawyers, and community representatives may be useful in obtaining buy-in, facilitating communication among stakeholders, and revising the policy in response to issues that develop.
The identification of hospital liaisons who have clear lines of authority and responsibility to work with police officers as conflicts or questions arise, since no policy can address all nuances of daily interactions in an ED. A liaison could minimize officer contact with patients and other hospital staff26 while decreasing the potential for traumatic interactions. Liaisons could be drawn from a number of departments, including social work or hospital security.
Development of trainings, using typical case scenarios, to raise ED staff awareness of hospital policies on law enforcement in the ED. Trainings should be mandatory and regularly updated as policy changes are made. Similar information sharing, including trainings, should also be crafted for police officers to ensure that they too are up to speed on new policies and their implementation.
Expanded access to legal consultation for clinicians. Many larger health care systems offer clinicians ways to contact legal counsel for assistance with the nuances of a specific situation, but such guidance is often lacking in smaller systems. It is important to ensure that clinicians are able to both follow the law and treat patients justly.
Simon, J. Derse, A. Marco, C., Allen, N., & Baker, F. Law enforcement information gathering in the emergency department: Legal and ethical background and practical approaches. Journal of the American College of Emergency Physicians Open, 4(2). https://doi.org/10.1002/emp2.12914
Janeway H., Samra S., & Song J. (2021). An Ethical, Legal, and Structural Framework for Law Enforcement in the Emergency Department. Annals of Emergency Medicine, 78(6), 749–751. https://doi.org/10.1016/j.annemergmed.2021.08.009
Alur R., Hall E., Khatri U., Jacoby S., South E., & Kaufman E. (2022). Law Enforcement in the Emergency Department. JAMA Surg, 157(9), 852–854. doi:10.1001/jamasurg.2022.2595
Khatri U., Kaufman E., Seeburger E., Alur R., Richardson L., South E., & Jacoby S. (2023). Emergency Medicine Physician Observations and Attitudes on Law Enforcement Activities in the Emergency Department. Western Journal of Emergency Medicine, 24(2). https://doi.org/10.5811/westjem.2022.12.57098
Kaufman, E., Khatri, U., Hall, E.., Alur, R., Song, J., & Jacoby, S. (2023). Law enforcement in the Trauma Bay: A Survey of Members of the American Academy for the Surgery of Trauma. Trauma Surgery & Acute Care Open, 8(1). https://tsaco.bmj.com/content/8/1/e001022
Khatri U., Kaufman E., Seeburger E., Alur R., Richardson L., South E., & Jacoby S. (2023). Emergency Medicine Physician Observations and Attitudes on Law Enforcement Activities in the Emergency Department. Western Journal of Emergency Medicine, 24(2). https://doi.org/10.5811/westjem.2022.12.57098
Kaufman, E., Khatri, U., Hall, E.., Alur, R., Song, J., & Jacoby, S. (2023). Law enforcement in the Trauma Bay: A Survey of Members of the American Academy for the Surgery of Trauma. Trauma Surgery & Acute Care Open, 8(1). https://tsaco.bmj.com/content/8/1/e001022
Jacoby, S., Kaufman, E., Richmond, T., & Holena, D. (2018). When Health Care and Law Enforcement Intersect in Trauma Care, What Rules Apply?. Health Affairs. doi: 10.1377/hblog20180926.69826
Kaufman, E., Khatri, U., Hall, E.., Alur, R., Song, J., & Jacoby, S. (2023). Law enforcement in the Trauma Bay: A Survey of Members of the American Academy for the Surgery of Trauma. Trauma Surgery & Acute Care Open, 8(1). https://tsaco.bmj.com/content/8/1/e001022
Khatri U., Kaufman E., Seeburger E., Alur R., Richardson L., South E., & Jacoby S. (2023). Emergency Medicine Physician Observations and Attitudes on Law Enforcement Activities in the Emergency Department. Western Journal of Emergency Medicine, 24(2). https://doi.org/10.5811/westjem.2022.12.57098
Tatebe, L., Kaufman, E., Nappi, T., Dennis, A., Neely, K., Hall, E., Smith, M., & Duncan, T. (2023). Walk the Line: An Ethical Framework for Interactions With Law Enforcement in Trauma Care Environments. Journal of Trauma and Acute Care Surgery, 94(2), 20–22. doi: 10.1097/TA.0000000000003810
Khatri U., Kaufman E., Seeburger E., Alur R., Richardson L., South E., & Jacoby S. (2023). Emergency Medicine Physician Observations and Attitudes on Law Enforcement Activities in the Emergency Department. Western Journal of Emergency Medicine, 24(2). https://doi.org/10.5811/westjem.2022.12.57098
Kaufman, E., Khatri, U., Hall, E.., Alur, R., Song, J., & Jacoby, S. (2023). Law enforcement in the Trauma Bay: A Survey of Members of the American Academy for the Surgery of Trauma. Trauma Surgery & Acute Care Open, 8(1). https://tsaco.bmj.com/content/8/1/e001022
Gallen, K., Sonnenberg, J., Loughran, C., Smith, M., Sheppard, M., Schuster, K., Kaufman, E., Song, J., & Hall, E. (2022). Health Effects of Policing in Hospitals: A Narrative Review. Journal of Racial and Ethnic Health Disparities, 10, 870–882. https://doi.org/10.1007/s40615-022-01275-w
Bailey, J., Jacoby, S., Hall, E., Khatri, U. Whitehorn, G. & Kaufman, E. (2022). Compounding Trauma: the Intersections of Racism, Law Enforcement, and Injury. Current Trauma Reports, 8(3), 105–112. https://link.springer.com/article/10.1007/s40719-022-00231-7
Aronowitz, S., Mcdonald, C., Stevens, R., & Richmond, T. (2020). Mixed Studies Review of Factors Influencing Receipt of Pain Treatment by Injured Black Patients. Journal of Advanced Nursing, 76(1), 34–46. https://doi.org/10.1111/jan.14215
Addison, H., Richmond, T., Lewis, L., & Jacoby, S. (2022). Mental Health Outcomes in Formerly Incarcerated Black Men: A Systematic Mixed Studies Review. Journal of Advanced Nursing, 78(7), 1851–1869. https://doi.org/10.1111/jan.15235
Jacoby, S., Richmond, T., Holena, D., & Kaufman, E. (2018). A Safe Haven for the Injured? Urban Trauma Care at the Intersection of Healthcare, Law Enforcement, and Race. Social Science & Medicine, 199, 115–122. https://doi.org/10.1016/j.socscimed.2017.05.037
Bruce, M., Ulrich, C., Webster, J., & Richmond, T. (2022). Injured Black Men’s Perceptions of the Recovery Environment. Social Science & Medicine, 292, https://doi.org/10.1016/j.socscimed.2021.114608
Even With Lower Prices, Medicare, Medicaid, and Other Insurers Tighten Coverage for Drugs Like Mounjaro and Zepbound Using Prior Authorization and Other Tools
A 2024 Study Showing How Even Small Copays Reduce PrEP Use Fueled Media, Legal, and Advocacy Efforts As Courts Weighed a Case Threatening No-Cost Preventive Care for Millions